Gait assessment is used to plan, and treat individuals with conditions affecting their ability to walk.
The gait cycle can start when one foot contacts the ground. If it starts with the right foot contacting the ground, then the cycle ends when the right foot makes contact again.
For the Components of the Gait Cycle , scroll below:
For Abnormal Gaits, see Abnormal Gaits page
Measurable Determinants for Gait Assessment:
- Width of Base: 2-4 inches. Straight distance between the feet (side to side) when walking. Wider Base – when patient is dizzy, inner ear problems, cerebral problems
- Normal Step Length: around 15 inches – the distance from the heel of the front foot & the toe of the back foot.
- Out Toeing: 8-10 º (degrees)
- Pelvis/ Trunk Shifts Laterally around 1 inch towards the weight bearing side
- Center of Gravity just anterior to S2 – during the gait cycle, the center of gravity moves laterally about 2 inches
- During the Swing Phase, the pelvis rotates 40º (degrees) forward
- Knee is flexed during all components of stance phase except on heel strike
- Average = 90 to 120 steps per minute
Visual Inspection of Gait Patterns:
HEAD & NECK MOVEMENT:
- Normal: slight movement
- Abnormal: bobbing forward, side to side, stiff posture, tilted
ARM MOVEMENT:
- Normal: pendulum (moving at the sides)
- Abnormal: arm cuts across the front of the body, shoulder internally rotated, no movement, one arm moving more than the other
LOWER BACK MOVEMENT:
- Normal: ASIS (anterior superior iliac spine) points forward – flex and extends
- Abnormal: lateral/side to side/rotary movements
LEGS & FEET:
- Normal: 8-10º out toe; legs straight
- Abnormal: scissors gait, internal and external rotation, valgus & varus at the knees
Gait Assessment
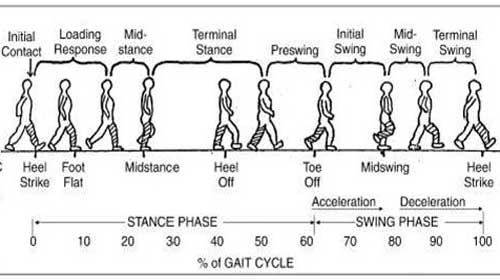
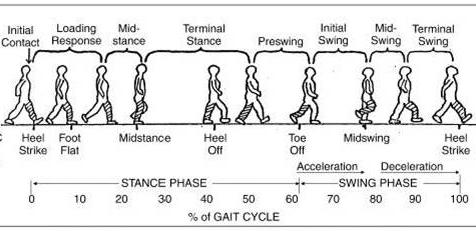
There are two phases of the gait cycle. Stance phase is the part of the cycle when the foot is in contact with the ground. It comprises 62% of the cycle, beginning with initial foot strike and ending with toe-off. Swing phase occurs when the foot is in the air and comprises 38% of the cycle, beginning with toe-off and ending with second (ipsilateral) foot strike.
The Gait Cycle: GAIT PHASES
A. STANCE PHASE
– Most problems with the gait occurs in the stance phase. This is the weight bearing component of the Gait Cycle.
Components / Parts of the Stance Phase:
- Heel Strike
- Foot Flat
- Midstance
- Push Off ( Toe Off)
1. Heel Strike – when the anterior compartment of the lower leg (quads) is contracting.
Gait Assessment on Heel Strike Issues:
- Pain in the presence of Heel Spurs, Calcaneal Bursitis, Achilles Tendonitis. To avoid pain, the patient hops or avoid heel strike altogether
- Weak quads will make the patient unable to extend the knee and may manually push the knee into extension
2. Foot Flat – foot moves into plantar flexion via the eccentric contraction of the anterior compartments of the lower leg. Knee and Hips are normally slightly flexed during in this component of the gait cycle.
Gait Assessment on Foot Flat Issues:
- Slap Foot/ Drop Foot – can be due to paralysis or weakness of the anterior compartment of the lower leg
3. Mid Stance – weight should normally be distributed to all aspects of the foot. Knee is normally in mild flexion, moving into extension/
Gait Assessment on Mid Stance Issues:
- Pes Planus – flat feet, fallen arches, subtalar arthritis – pain when waling on uneven ground
- Painful Callouses at the metatarsal heads
- Plantar Warts
- Osteoarthritis – most painful on midstance
- Weak Quads – excessive knee flexion or unstable knee
- Weak Gluteus Medius – trendelenbergs gait; gluteus medius lurch
- Weak Gluteus Maximus -thorax thrust posteriorly to maintain hip flexion
4. Push Off/ Toe Off – Gastrocnemius and Soleus contracting, occurs at the ball of the foot ( 1st metatarsophalangeal – MTP joint), knee is slightly flexed and hip is extended.
Gait Assessment on Push Off Issues:
- Pain during push off- compensating by Toe off from lateral edge of foot instead – can be caused by Osteoarthritis or fused MTP joint, also hallux valgus
- metatarsalgia
- soft corns between 4th and 5th toes
- weak plantar flexors (gastrocs/soleus) – flat footed gait or calcaneal gait – no forceful toe off
B. SWING PHASE
Components / Parts of the Swing Phase:
- Acceleration
- Midswing
- Decceleration
* DROP FOOT – is a problem for the entire swing phase (weak anterior compartment)
1. Acceleration – foot is normally dorsiflexed to clear the ground. Knees moving into flexion. Hip moves from hyperextension to mild flexion.
Gait Assessment on Acceleration Issues:
- drop foot
- weak hamstrings – lack of knee flexion ( cannot clear the ground)
2. MidSwing – foot is also normally dorsiflexed to clear the ground.
Gait Assessment on Midswing Issues:
- weak dorsiflexors – patient trips all the time; scratch at the toe of patient’s shoes, toe scrapes the ground – to compensate = uses steppage gait.
3. Decceleration – foot is normally dorsiflexed, knee is normally in flexion moving into extension; hamstrings eccentrically contacting to slow down the swing prior to heel strike.
Gait Assessment on Decceleration Issues:
- drop foot
- weak hamstrings – excessively harsh heel strike
For Abnormal Gaits, see Abnormal Gaits page